


Heartbroken
Analysis by Claus Rinner - 9 February 2022.
There are many reasons to be heartbroken at the tail end of the corona crisis. Families have lost loved ones in isolation, and possibly due to isolation. Young people died tragically and unnecessarily from COVID—thanks in part to the suppression of effective treatment protocols—or from drug overdoses—quite possibly a result of their lives being turned upside down by the pandemic response measures. And 2021 all-cause mortality increased in concert with the ramping up of COVID-19 vaccination programs in many countries. In addition to death, heart disease is one of the many known adverse event of the injections.
In its weekly report on “adverse events following immunization” (AEFI), Public Health Ontario (PHO) monitors safety signals during the rollout of the inoculations. Inflammation of the heart (myocarditis and pericarditis) is an “adverse events of special interest” (AESI) for PHO. In September 2021, Ontario’s Chief Medical Officer of Health had issued a “preferential recommendation” for the Pfizer product over Moderna for young males aged 18-24, later expanded to the male teenager group aged 12-17. This decision was likely based on PHO’s “Enhanced Epidemiological Summary” covering data up to 4 September 2021. For the “enhanced surveillance period” of June, July, and August 2021, that document specifies a myo/pericarditis reporting rate of 262.1 per million, or 1 in 3815, in 18-24 year-olds based on a total of 37 reports for dose 2 of the Moderna product, with a much lower 47.3 per million, or 1 in 21142, based on a total of 58 reports for dose 2 of Pfizer. Media reports at the time pegged the risks at 1 in 5000 for Moderna, compared to 1 in 28000 for Pfizer.

Citizen researcher Koen Swinkels published a detailed analysis on 1 October 2021, in which he concludes that “Public Health Ontario Is Not Being Honest about the Myocarditis Risk in Young Males“, because more recent data showed even higher rates than those cited for the “preferential recommendation”. Based on research in Israel, Swinkels estimated an under-reporting factor of 3 on top of the above calculations and recommended the immediate stop of the youth vaccination campaign.
Fast forward to the current PHO AEFI report with cumulative data until 30 January 2022, and we see a crude reporting rate for myo/pericarditis (Table A3, page 29) of 199.7 per million, or 1 in 5008, in 18-24 year-olds for dose 2, based on a total of 660 reports. This rate predominantly represents Pfizer shots administered after the “preferential recommendation”, yet it is at the level for which the recommendation against the Moderna product was issued. To make matters worse, if we consider that each young adult is supposed to receive dose 1 and dose 2, the total risk for getting “fully vaccinated” (but not “boosted”) adds up to 251.2 per million, or 1 in 3981. For the male teenager group, the total risk amounts to 219.7 per million, or 1 in 4552. Add in the under-reporting issue, as well as subclinical, non-hospitalized cases, of which I personally know two and another three indirectly, and you obtain risks in the order of 1 in a few hundred, which turns heart inflammation into an “uncommon”, rather than “rare”, adverse event from COVID-19 injections.
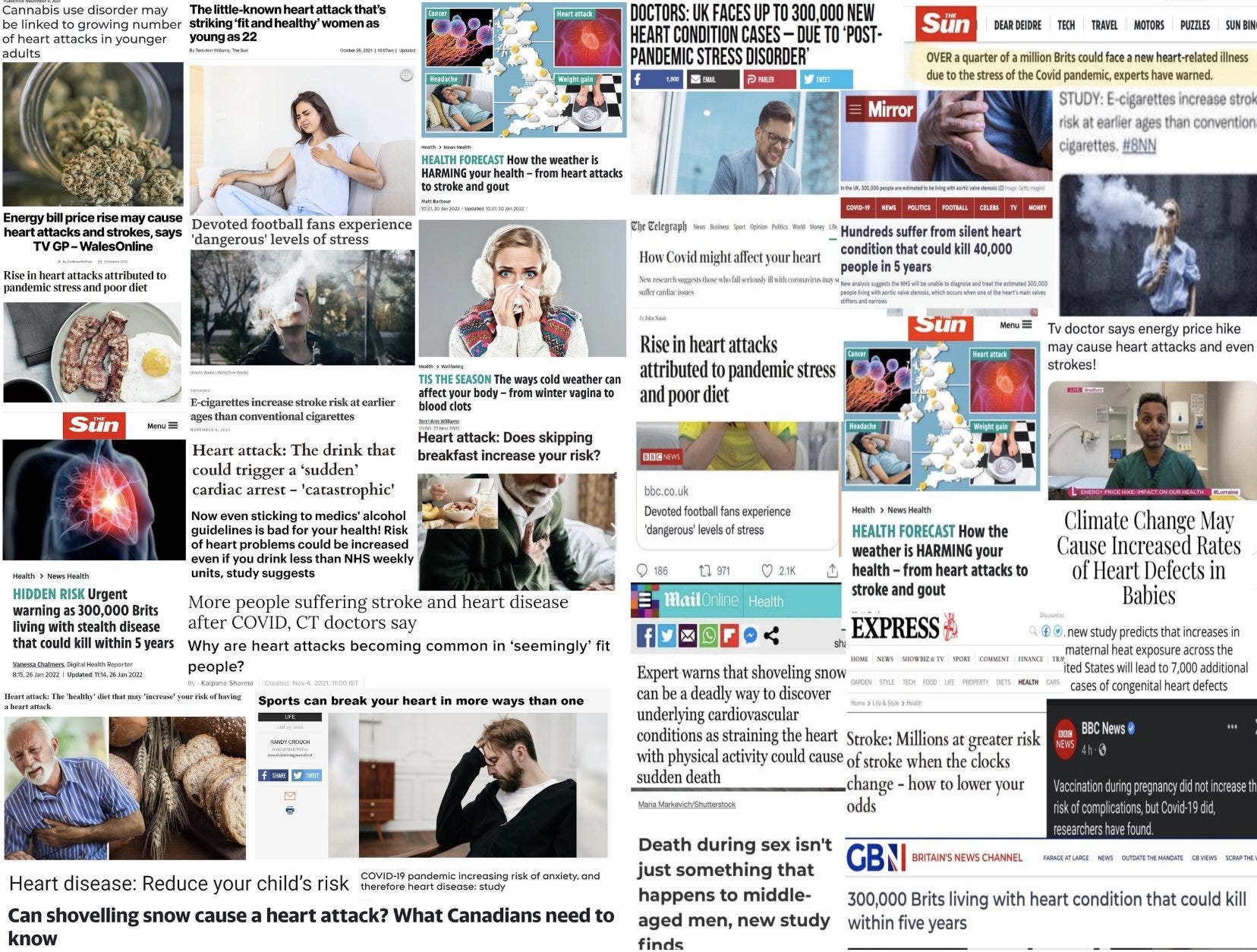
Thanks to my well-informed Twitter bubble, I have started to see numerous media reports about increasing heart issues in the population. And about the possible reasons. These include:
cold weather
warm weather
climate change
skipping breakfast
eating a healthy breakfast
watching soccer
playing soccer
…and many more!
One widely shared news item read “Shaking duvet too vigorously while making your bed can increase your chances of a heart attack, scientists warn.” Sadly, fact checkers will mercilessly debunk just about any good story … in this case, an eagle-eyed Snopes writer noticed an irregularity in the picture that came with the story. Snopes cleverly uncovers the motivations behind sharing the deadly duvet shaking story, namely:
“These posts falsely argued that the media was attempting to disguise an increased risk of heart attacks from the COVID-19 vaccine by publishing a wave of articles blaming other factors (such as rigorously shaking a duvet cover) for heart attacks.”Of course, the fact check then throws in some disconnected bits of disinformation purportedly showing the greater benefit of the injections in preventing COVID-induced heart problems as compared to the vaccine-induced heart issues. Yet, they conflate the likelihood of heart problems in patients hospitalized for or with COVID-19, without reference to their age distribution, with the myo/pericarditis risk in teenagers, here pegged at 1 in 6000. They also claim categorically that “These cases have been mild and self-resolving”, while PHO reports (Table 1, page 6) that 96% of acknowledged myo/pericarditis cases went to emergency and 66% stayed in hospital, hardly indicating a mild illness.
Whether the frequency of health reports in the legacy media is indeed higher than usual, and could be part of a campaign to normalize heart issues, will be difficult to prove. But the use of the mass media to nudge the population into compliance with pandemic restrictions is well established. Nudging our attention away from concerning public health trends would be a logical next step. And it is clear that many Canadians suffer from literal or metaphorical “broken heart symptom” and “post-pandemic stress disorder” causing cardio-vascular issues. That’s yet another reason for a great reset of public health—back to a holistic perspective on health as a complex system of interconnected individuals, environments, and circumstances that can be supported gently but never mechanistically controlled.
Shocking CDC campaign to normalize blood clots in healthy athletes, with a comment from Dr. Simone Gold, founder of America's Frontline Doctors - https://twitter.com/drsimonegold/status/1492901677959106560